|
Welcome to TRVN: QuickStart
|
Discover drop down menus above for items such as:
|
This video answers nearly all the questions about the product benefits, product launch, and other pipeline assets.
Trevena, Inc. Oppenheimer Fall Healthcare Life Sciences & MedTech Summit Virtual September 23, 2020 11:40 a.m. ET
(Click the button below, then take a moment and "Register" to gain access)
Trevena, Inc. Oppenheimer Fall Healthcare Life Sciences & MedTech Summit Virtual September 23, 2020 11:40 a.m. ET
(Click the button below, then take a moment and "Register" to gain access)
Overview:
Trevena (NASDAQ: TRVN) is a clinical stage biotech company based in Pennsylvania w/ approx. 20 employees. The founders Robert Lefkowitz is a Nobel Prize recipient and as "many as 30 to 50 percent of all prescription drugs are designed to "fit" like keys into the similarly structured locks of Lefkowitz' receptors—everything from anti-histamines to ulcer drugs to beta blockers that help relieve hypertension, angina and coronary disease."
Main Asset - Olinvyk (TRV130: Oliceridine):
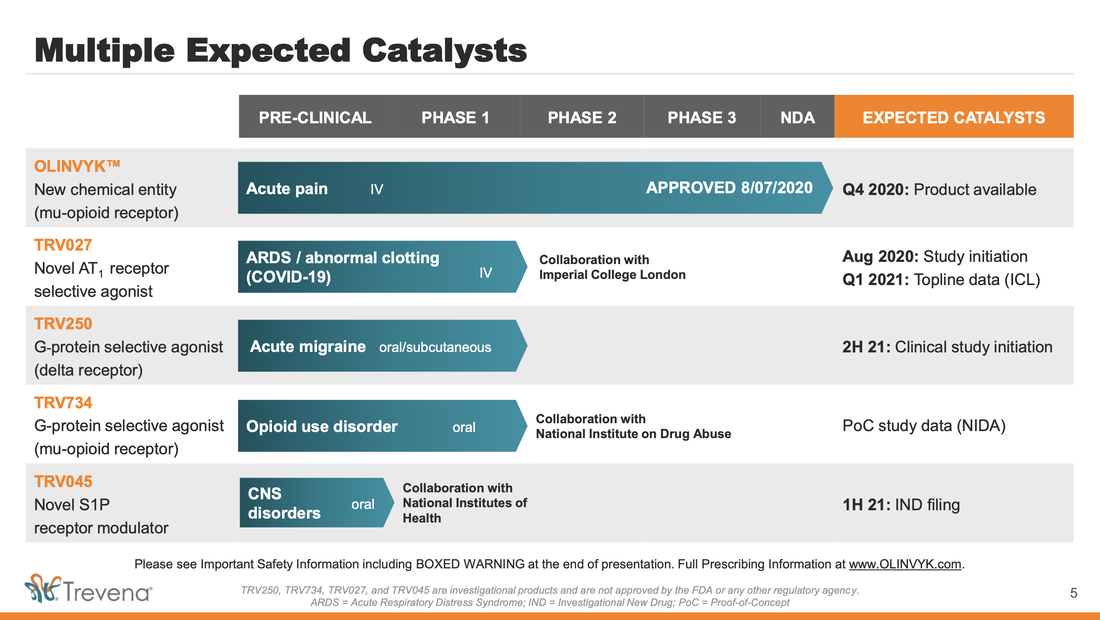
Trevena's Olinvyk (new. chemical entity / mu-opioid receptor) received FDA on 08/07/2020. DEA classification for drug Scheduling will occur no later than 90 days after FDA approval (on or before 11/07/2020).
Pipeline:
There is a treasure trove of data supporting each of the pipeline asset below. Due to space constraints and comprehension/functionality, please Google any questions or ask a Stocktwits member on the TRVN board.
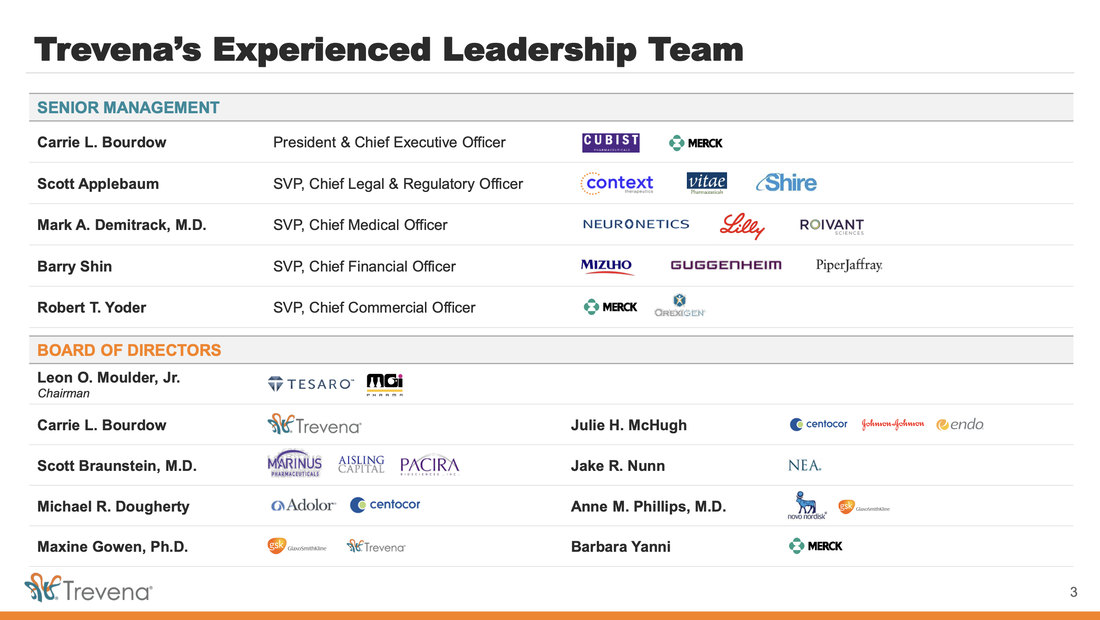
Management:
Hear the voices of Trevena's mgt. by listening to the Q1 2020 Earnings Conference Call w/ the links at the bottom of this page:
Near-team catalyst:
1) Price target upgrades from underwriters
2) TRV027 updates
3) Syneos PR
4) Early DEA scheduling
5) TRV045 data from NIH
6) Coverage from a respected firm such as Oppenheimer
7) A South Korea milestone pmt before Nov. earnings reports
8) Update of TRV045
2) TRV027 updates
3) Syneos PR
4) Early DEA scheduling
5) TRV045 data from NIH
6) Coverage from a respected firm such as Oppenheimer
7) A South Korea milestone pmt before Nov. earnings reports
8) Update of TRV045
|
Be sure to explore both links in the post above!
|
|
Earning:
Q1 2020 Earnings Results
I recommend listening to the actual call (24 minutes, 54 seconds). Go to Trevena to register and to listen:
https://www.trevena.com/investors/press-releases/detail/228/trevena-reports-fourth-quarter-and-full-year-2019-results
Trevena, Inc. (NASDAQ:TRVN) Q1 2020 Earnings Conference Call May 7, 2020 8:00 AM ET
Company Participants
Robert Yoder - Senior Vice President and Chief Business Officer
Carrie Bourdow - President and Chief Executive Officer
Mark Demitrack - Senior Vice President and Chief Medical Officer
Barry Shin - Senior Vice President and Chief Financial Officer
Conference Call Participants
Jason Butler - JMP Securities
Douglas Tsao - H.C. Wainwright & Co., LLC
Operator
Ladies and gentlemen, thank you for standing by, and welcome to the Trevena, Inc. First Quarter Earnings Conference Call. At this time, all participants are in a listen-only mode. After the speaker presentation, there will be a question-and-answer session. [Operator Instructions] Please be advised that today’s conference is being recorded. [Operator Instructions]
I would now like to hand the conference over to your speaker today, Mr. Bob Yoder, Chief Business Officer. Thank you. Please go ahead, sir.
Robert Yoder
Good morning, and welcome, everyone. Thank you for joining us on this morning's call. With me today are Carrie Bourdow, our President and CEO; Mark Demitrack, our Chief Medical Officer; and Barry Shin, our Chief Financial Officer.
Before we begin, we wish to inform participants that we will be making forward-looking statements on this call, which are made pursuant to the safe harbor provision of the Private Securities Litigation Reform Act of 1995.
You are cautioned that forward-looking statements involve risks and uncertainties, including risks detailed from time-to-time in the Company's periodic reports filed with the Securities and Exchange Commission, and we undertake no obligation to update these statements beyond today.
During today's call, Carrie will give some opening remarks on our progress of oliceridine and I'll provide an overview of our commercial launch strategy. Mark will then provide some additional details on our ongoing pipeline activities and Barry will review our financial results followed by some time for questions.
I'll now turn the call over to Carrie.
Carrie Bourdow
Thank you, Bob. Good morning, everyone. Thank you for joining us today. I hope that you and your families are staying safe during these unprecedented and challenging times. I would like to open the call this morning by extending my many thanks to the healthcare professionals, our employees, and our business partners who help us move forward in our commitment to patients.
Like a lot of you, we are watching the COVID situation closely and while our priority of course is on the health and safety of our employees and our communities, I am also very grateful that we've been able to remain resilient and focused on business continuity.
And to that end, let me provide a few highlights on our lead asset IV oliceridine. As you all know, we have a PDUFA date for oliceridine of August 7, and it's clear to us that the agency is active in the review of our resubmission. I am very pleased with FDA's engagement, and we expect FDA's review of our application to continue on track. We are looking forward to receiving their decision in August.
At the same time, we are working to ensure that after approval and DEA scheduling, we can make oliceridine available to hospitals and healthcare providers in the fourth quarter of this year. Our commercial manufacturing facilities, which are located in the U.S. are manufacturing drug product as we speak.
We are also actively investigating collaborations and strategic partnerships to support the U.S. commercial launch of oliceridine and our current ex-U.S. partners are making progress on their regulatory timelines. Our top priority is getting oliceridine to acute pain patients and we are exploring all options to help us maximize shareholder value as we do this.
So now let me turn the call over to Bob, who will go into more detail on our U.S. commercial strategy. Bob?
Robert Yoder
Thank you, Carrie. Well, this is certainly an exciting time for us as we continue preparations for the commercial launch of oliceridine, either by ourselves or with a partner. As you'll hear me layout, our strategy is built around focus and efficiency, targeting the right patient population, physician specialties and accounts in order to facilitate initial uptake.
The market opportunity is large with approximately 45 million patients each year who receive drugs like IV morphine for acute pain. Additionally, the overall size of the market in terms of unit sold has remained relatively stable over the last 18 months, suggesting that potent analgesics such as IV morphine are still needed in the hospital settings.
The product profile oliceridine when compared to IV morphine, it's differentiated in a number of key areas. Unlike morphine, oliceridine has a fast onset of two to five minutes, no known active metabolites and no dosage adjustment needed in elderly or renally impaired patient.
Oliceridine offers a compelling set of attributes that address the unmet needs that still remain to both the inpatient and outpatient settings. We know that roughly 20% of the overall hospital patient population are considered high-risk for adverse effects, including patients with certain comorbidities, obese patients, those with renal impairment and the elderly.
We refer to this subset as our core patients. Physicians continue to face particular challenges in effectively and safely treating these patients and those challenges have unfortunately been highlighted by the ongoing pandemic.
In ATHENA, our open-label, real world safety study published last year, we studied many of these high-risk patients across a range of surgical settings. In fact, 30% of patients were over the age of 65 and 50% were clinically obese.
You may recall during our last earnings call in March, Dr. Tim Beard, a colorectal surgeon practicing in Oregon described patient types very similar to those we study, who he felt might benefit from a drug such as oliceridine.
Our launch strategy is focused and targeted. The core patients I described earlier will be our initial focus as those patients currently present the greatest difficulty in pain management. We also plan to concentrate initially on a subset of physician specialties, anesthesiologist, colorectal, orthopedic, and cardiothoracic surgeons.
These specialties have a high volume of procedures in which multimodal pain management, protocols frequently required drugs such as IV morphine. These facilities are also treating a high number of our core or high-risk patients. Finally, we plan to focus on a subset of hospitals and outpatient surgery centers that have demonstrated early adoption of other branded agents in the past.
Of course, we are closely monitoring the impact of the current pandemic and how that could change our thinking about our commercialization strategy. But we continue to hear about high-risk patients, the challenges these patients present in effective pain management and growing pent-up demand created by pauses and procedures considered to be elective surgeries and exacerbated by the current shortage of drugs like IV morphine.
In closing, we are taking an approach to commercialization that is all about focus. The right group of patients treated by a targeted subset of physician specialties and within a group of hospitals and surgery centers where we believe the potential oliceridine is significant.
Let me now turn the call over to Mark to provide some additional details on our pipeline activities.
Mark Demitrack
Thank you, Bob. Let me start with some additional comments on oliceridine. I am pleased to report that we've continued to add to the body of peer-reviewed literature, which is an important element supporting the launch strategy that Bob just outlined.
We recently announced the publication of a comprehensive review of the non-clinical and clinical data for oliceridine. In addition, I would like to highlight the online publication of a poster in association with this year's ASRA meeting.
The poster is titled Low Incidence of Opioid-Induced Respiratory Depression in High-Risk Elderly Obese Patients. This report summarizes the findings of a post-hoc analysis of data from an ATHENA study. We compared the incidence of clinical indices of respiratory depression across two patient subpopulations in that study.
Those considered high-risk and those considered low-risk. High-risk patients were those individuals who were over 65 years old and had a BMI greater than 30. As Bob mentioned earlier, these patients were a large proportion of the study population. Low-risk patients were defined as the opposite, those younger than 65 with a BMI less than 30. The results were very interesting to us.
The incidence of respiratory depression was similar in both groups, despite the high-risk group being defined by two characteristics known to raise the risk of respiratory complications during treatment with conventional medications like IV morphine.
These data are consistent with feedback we received from investigators during the ATHENA study on their assessment of oliceridine's distinctive clinical profile. These data will serve as an important point of departure for our thinking about future research.
Beyond oliceridine, we continue to make good progress with our pipeline for TRV045, our novel S1P receptor modulator. Our collaboration with NIH is ongoing and productive. They've initiated the first round of non-clinical studies in their epilepsy screening program and we look forward to reporting on that work in the future.
Most of us announced this morning that NIH plans to begin evaluating TRV045 within another screening program. This one designed to study novel non-addictive treatments for pain. This program is based on the longstanding epilepsy screening program, which is viewed as a highly successful partnership model and also features a rigorous evaluation process for entry.
The program includes assays and models of acute, inflammatory and neuropathic pain, all of which were funded by NIH. The fact that TRV045 has received such interest from NIH, I believe speaks to its exciting promise as a novel approach to treating a variety of CNS disorders.
I look forward to working closely with NIH to further explore the therapeutic potential of this asset. In parallel with these activities, we continue to make progress on our own IND-enabling work with this compound, and I am very pleased to announce that we are now planning on filing an IND application for TRV045 in the first half of 2021.
I'd now like to turn it over to Barry for review of our Q1 financials. Barry?
Barry Shin
Thanks, Mark. We issued a press release. We filed our Form 10-Q with our full financial results. For now, I'll summarize the headline numbers. For the first quarter of 2020, we had a net loss of $5.7 million or $0.06 per share, compared to $5.2 million or $0.06 per share for the first quarter of 2019. This increase in net loss is mainly due to higher R&D expenses associated with a TRV250 acute migraine proof-of-concept study and activities to support the NDA resubmission for oliceridine.
As of March 31, 2020, we had cash and cash equivalent of $28.1 million, which reflects the full repayment of our term loan on March 2. We continue to expect that this amount will fund our operations and capital expenditures into the first quarter of 2021. This includes the expected approval of oliceridine in August and post-approval activities to ensure oliceridine as commercially available in the fourth quarter of 2020.
We'll now open the call for questions, after which Carrie will provide some closing remarks. Rachel?
Question-and-Answer Session
Operator
[Operator Instructions] Your first question comes from the line of Jason Butler. You may begin.
Jason Butler
Thanks for taking the questions. First one on oliceridine, can you just give us any color around manufacturing inspection? Did you have a pre-approval inspection during the first cycle NDA review? And do you expect that any additional inspections to be needed by FDA before your PDUFA date?
Carrie Bourdow
Good morning, Jason. Thanks for the question. We did not have previously an inspection, but the – so I mentioned the sites are in the U.S., the API and drug product sites are in the U.S., which we think is a good thing. And they have been inspected last year for other products, didn't have any issues, no 483, so we're not anticipating manufacturing is going to be a problem at all for us.
Jason Butler
Okay. Great. You ran through some of the patients you're targeting – the high-risk of adverse events and the physicians as well. As you think about the beginning of a resumption of elective procedures, where is the overlap and how do you think about the dynamics of which procedures could ramp sooner and where we could see a prolonged proponent procedures and ultimately are you looking to refocus any of your launch strategy in response to these dynamics? Thanks.
Carrie Bourdow
Yes. So I'll let Bob address this. But let me just say that we're talking with a lot of our key opinion leaders across the country and it's not necessarily, which procedures may start kicking in sooner. It's really based on geography in some cases.
Our core areas, as Bob mentioned, cardiothoracic, colorectal, orthopedic, certainly cardiothoracic, we believe will start happening sooner, and of course, like everyone are sort of thinking through what our launch strategy will look like.
Let me just brag on Bob really quickly before I turn it over. So one of the reasons we asked Bob to join Trevena is that he has a lot of experience in non-personal promotion launches, launching with more of a digital focus. I think that's going to serve us well when we sort of think through our launch strategy. But Bob, any additional comments?
Robert Yoder
Sure, yes. Hi, Jason. Thanks for the question. So one thing I'd say about the procedures piece of it, is the things I'm reading at least say as an elective procedures that were paused or canceled or coming back online.
What I've been reading is that the patient type that they're looking to prioritize are typically those higher risk patients because often times that profile just gets riskier with time. So they're trying to in many cases push those high-risk patients to the front of the queue as those procedures come back.
Around the strategies, obviously we're watching very closely what the pandemic is doing to HCP engagement. In this case, I think the early trends seem to suggest that physicians are engaging remotely a little more. They're open to that more. Digital channels are getting more robust as well.
So I think, overall, an effective engagement on the future of what we're going to be thinking about is likely, the flexibility to dial up or dial back a wider array of channels, digital channels, non-personal promotion and things like that. Certainly, until we see what will happen with traditional face-to-face access with HCPs over time. But definitely we're going to keep an eye out and think creatively about how we're going to engage with HCPs and what – I guess will be the new normal going forward.
Jason Butler
Great. And then just one more for me on 045, obviously the work being done at NIH, can you discuss or point to any additional preclinical work that you guys need to do in-house to support the IND filing in the first half of next year? Thanks.
Carrie Bourdow
Yes. Thanks, Jason. Mark, you want to talk a little bit about…
Mark Demitrack
Sure, Jason. So our [indiscernible] activity really revolves around much of the conventional components with any IND that we need to be assembled. So we have to obviously proceed with the necessary tax work and the manufacturing readiness that we needed for the formulation that we would bring into human use. So those programs are proceeding as I mentioned on plan at this time.
Jason Butler
Okay. Great. Thanks for taking the questions.
Carrie Bourdow
Thanks, Jason. Any other questions operator? Rachel?
Operator
Your next question comes from the line of Douglas Tsao. You may ask your question.
Carrie Bourdow
Good morning, Doug.
Douglas Tsao
Good morning. Just you maybe first touch on a little bit and obviously you've spoken about sort of some of the delays and sort of the backlog and intellective procedures, just sort of the context of the shortages that seem to be taking place for a lot of IV pain medications, just given the demand placed on hospitals because of COVID, and does that affect your launch strategy in anyway? And then also and I might have missed it, a lot going on in the household this morning.
Carrie Bourdow
Yes.
Douglas Tsao
Just in terms of the pause for TRV250 and when you might be able to get that started again?
Carrie Bourdow
Yes. So let me handle that first and then I'll turn the question over to Bob around some of our additional commercial strategy. So on TRV250, as you mentioned, we are on pause. That study is being conducted in the UK. And like everyone, we're sort of watching and having conversations with the clinical site in the UK.
So as soon as they feel comfortable to get moving again, we'll be doing that, but we don't have any additional guidance on that. We removed the timing guidance on TRV250. But we are having active conversations with the clinical site. So it's good.
Bob, do you want to – I know you talked a little bit about the commercial strategy in COVID and COVID patients, but any other additional comments you want to make certainly with the focus around high-risk patients in COVID? We've always been focused in high-risk patients, but there's a heightened sensitivity of what happens when those patients get sick in the hospital. So I don't know if you want to talk a little bit more about that.
Robert Yoder
Yes. Hi, Doug. I mean, I think you're right. You're pointing out definitely that's the – there's many unfortunate things around the pandemic and certainly one of them is [indiscernible]. We've all seen now that these high-risk patients present a lot of challenges in clinical management.
Specific to your question around the shortage too, I mean, I think, there is some data out there publicly [indiscernible] talked about at least within March, maybe the first part of April even that there is a pretty significant shortage. I think fill rates were hovering in the 70% range for IV opioids-driven. I think a lot I use in COVID patients, incubated patients. But the other impact of that is that that leaves – that’s available for use in post-surgical moderate to acute pain – moderate to severe pain.
So I mean, I think, I don't know beyond what I said before Doug in terms of change of strategies, it certainly tightens our urgency to be prepared for a really successful launch and get the product out there. So that compelling profile is in the hands of our physicians and they can use it where it's indicated, where they see fit.
Douglas Tsao
And maybe as a follow-up, I know it's still obviously very early days, and you're sort of limited in what you can do in terms of gauging with clinicians at this point. But just curious if you've gotten feedback from people sort of anxious to get it, because obviously I think the COVID-19 crisis has really sort of exposed the vulnerability of the American Healthcare System from a capacity standpoint.
Are you getting feedback that sort of greater interest in oliceridine because that's certainly one of the attributes of the product is really to sort of help improve efficiency of the system, which perhaps I think we probably took for granted before this sort of took place.
Carrie Bourdow
Yes. It's a really good point. I mean, I think we've talked before about the – in particular the investigators that were involved in ATHENA are interested in getting oliceridine, having oliceridine has an alternative. We're three months away from PDUFA date. So I think that's – they're excited about that potential opportunity of having oliceridine here relatively soon.
I do agree with you. I think, as I mentioned earlier, in particular the high-risk patients, right. Well we've talked about, you've heard us talk about is when these patients get sick, they stay even longer in the hospital. They put a lot of cost into the hospital system, some of the hardest, most difficult patients to treat.
So it's been a focus of ours since the beginning to focus on those patients. That's where we think we'll get the initial use for oliceridine. Beyond that, as it relates to COVID, I think we're all sort of watching things and staying focused on getting oliceridine approved by the agency.
Douglas Tsao
Okay. Great. That's it for me. Thank you.
Carrie Bourdow
Thank you, Doug. Appreciate it.
Operator
I am showing no further questions at this time. I would now like to turn the conference back to Carrie Bourdow, CEO.
Carrie Bourdow
Great. Well, thank you all. I appreciate all of the questions this morning. And as you can hear, we are optimistic and excited about oliceridine and PDUFA date that is quickly coming up. We are also excited about TRV045 and the NIH interest in 045 and also the progress that we've made in our IND capabilities and the ability to have an IND hopefully in the first half of next year.
So thank you again for the time despite all the craziness that we're all dealing with. As you hear, we are passionate about our mission in developing novel medicines for patients in need. Thank you again for joining us this morning.
Operator
Ladies and gentlemen, this concludes today's conference call. Thank you for participating. You may now disconnect.
Q4 2019 Results Earnings
Conference Call March 12, 2020 8:00 AM ET
I recommend listening to the actual call (33 minutes, 59 seconds). Go to Trevena to register and to listen: https://www.trevena.com/investors/press-releases/detail/228/trevena-reports-fourth-quarter-and-full-year-2019-results
Trevena, Inc. (NASDAQ:TRVN) Q4 2019 Results Earnings Conference Call March 12, 2020 8:00 AM ET
Company Participants
Robert Yoder - Senior Vice President, Chief Business Officer
Carrie Bourdow - President and Chief Executive Officer
Mark Demitrack - Senior Vice President, Chief Medical Officer
Timothy Beard - Chair of the Department of Surgery, Summit Medical Group
Barry Shin - Senior Vice President, Chief Financial Officer
Conference Call Participants
Jason Butler - JMP Securities
Douglas Tsao - H.C. Wainwright & Co.
Operator
Greetings and welcome to the Trevena Fourth Quarter and Full-Year 2019 Earnings Call. At this time, all participants are in a listen-only mode. A brief question-and-answer session will follow the formal presentation. [Operator Instructions]. As a reminder, this conference is being recorded.
It is now my pleasure to introduce your host, Bob Yoder, Chief Business Officer. Please go ahead.
Robert Yoder (00:30)
Thank you and welcome, everyone. Thank you for joining us on this morning's call. With me today are Carrie Bourdow, our President and CEO; Mark Demitrack, our Chief Medical Officer; Barry Shin, our Chief Financial Officer; and Timothy Beard, Chair of the Department of Surgery at Summit Medical Group in Bend, Oregon.
Before we begin, we wish to inform participants that we will be making forward-looking statements on this call, which are made pursuant to the Safe Harbor provision of the Private Securities Litigation Reform Act of 1995. You're cautioned that such forward-looking statements involve risks and uncertainties, including risks detailed from time-to-time in the company's periodic reports filed with the Securities and Exchange Commission. And we undertake no obligation to update these statements beyond today.
During today's call, Carrie will review our 2019 and recent corporate achievements and lay out our plan for 2020. Mark will provide an overview of the data from our IV oliceridine program that was recently resubmitted to FDA. Dr. Beard has also joined us this morning to provide his perspective on the current role of IV opioid analgesics in his clinical practice. Barry will then review our financial results, followed by some time for questions.
I'll now turn the call over to Carrie.
Carrie Bourdow (01:43)
Thanks, Bob. Good morning, everyone. Thank you for joining us this morning. At the start of 2019, you'll remember that I laid out a plan to resubmit oliceridine for approval and to advance the pipeline.
What you're going to hear this morning on this call is that we've delivered on the plan and you'll hear that with successful resubmission of oliceridine, we'll now turn our attention to preparing for expected approval in August of this year.
And on the pipeline front, what you'll hear is that we've hit key development milestones. We now have two proof-of-concept studies underway – one for acute migraine and another for opioid use disorder. And we're studying TRV045, a novel S1P modulator in epilepsy and a variety of other CNS conditions.
Importantly, we completed all of this work while we managed our expenses very carefully. And I have to say I am extremely proud of this team and what was accomplished in 2019.
Let me give you just a few more details on the highlights, the high points from my perspective from the year. As you saw last week, FDA accepted our resubmission of the oliceridine NDA and it's crazy. They told us that it was a complete response to their action letter. They set a PDUFA date of August 7 and we're looking forward to working with them as they review our application.
In the past, you've heard me talk about the market opportunity for oliceridine. It's large. Over 45 million patients each year in US hospitals receive drugs like IV morphine for acute pain, and about 9 million of those patients are at greater risk of developing adverse events. Hospitals are seeing a rise in these at-risk patients and an increase in the number of severe acute pain surgery.
And we believe this at risk patient population alone represents a total addressable market of $1 billion to $1.5 billion. That's impressive.
But at the end of the day, it's important that we focus on why we developed a novel analgesic like oliceridine and the reason is to improve patients' lives. Later on this call, we've invited Dr. Tim Beard to talk with you about some of his high-risk patients and the challenges that he faces in managing post-op acute pain.
Beyond oliceridine, we made significant progress on the pipeline. Late last year, we initiated an acute migraine proof-of-concept study for TRV250. Migraine is also another large market. Approximately 650 million migraines are treated annually in the US. And there's still a need for novel treatment options.
TRV250 is a novel new mechanism, and this one at the delta receptor. And the delta receptor is located throughout the brain and the delta receptors regulate mood, anxiety and pain, including migraine pain. We're evaluating the ability of TRV250 to reduce the occurrence of headaches and also to potentially reduce symptomatic anxiety. About half of all migraine patients experience anxiety.
There are no approved treatment options that can treat both migraines and anxiety. So, obviously, this would be a large market opportunity for us for TRV250. It's a really exciting asset and we're expecting top line results on this study in the second half of this year.
Another proof-of-concept study we started late last year was in collaboration with the National Institute on Drug Abuse, or a group called NIDA. And this study is for TRV734 for opioid use disorder.
NIDA is looking at the potential of 734 as a safer and better tolerated treatment option for patients suffering from addiction. We're really pleased to be working with NIDA to help fight the opioid crisis and I'll keep you updated as the study progresses.
And then lastly, as you saw this morning, we announced that we've initiated another collaboration with the NIH to investigate the potential of TRV045 as a treatment for epilepsy. 045, another new mechanism, represents a novel approach to treating neurological disorders. And it's a next generation S1P receptor modulator that activates the receptor target without any of the immunosuppression that you get with other S1P modulators.
NIH has already initiated the first round of assays for epilepsy. And we believe this asset holds promise not only for epilepsy, but for a variety of CNS indications.
With all of our assets, including oliceridine, we're actively investigating collaborations and strategic partnerships. Remember, we already have two ex-US partnerships for oliceridine. And these collaborations are going really well. We're expecting to receive a $3 million milestone payment upon FDA approval of oliceridine.
As we continue to make progress on oliceridine and the pipeline, we're going to continue to look for ways to advance all of our assets and to maximize shareholder value.
With that, let me now turn the call over to Mark.
Mark Demitrack (07:12)
Thank you, Carrie. I'm also very pleased that we've successfully re-submitted our NDA for IV oliceridine. This milestone represents more than a year of work by members of our clinical, non-clinical, manufacturing and regulatory teams. And I'm extremely grateful for the opportunity to work with such a dedicated group of individuals.
I believe the outcome of that work is compelling and further strengthens our evidence in support of oliceridine as a potential new treatment option for patients with moderate to severe acute pain.
The promise of oliceridine as a distinctive addition to a clinician's armamentarium of IV analgesics is built on its novel mechanism of action and unique pharmacokinetic profile.
Oliceridine is a new chemical entity, a first in this space in decades, and was designed to optimize G protein coupled receptor pharmacology by preferentially engaging the G protein signaling pathway responsible for analgesia, with reduced recruitment of beta-arrestin, which is largely involved in development of adverse effects.
Oliceridine has a rapid onset of action, with perceptible pain relief as early as two to five minutes after the first dose and lasting approximately three hours, providing a highly differentiated analgesic profile for clinicians.
Oliceridine also has no evidence of active metabolites, which can complicate dosing and result in the emergence of delayed adverse events.
Finally, our recently published studies in special populations have shown that no dosage adjustment is necessary in patients with underlying renal impairment or in the elderly. These attributes distinguish oliceridine from currently available IV analgesics like morphine.
As a reminder, we've amassed a comprehensive clinical data set for oliceridine across multiple efficacy and safety studies, involving over 1,800 individuals.
On past calls, we've spoken about the respiratory safety data, but today I'd like to highlight the GI tolerability data collected during our pivotal Phase III studies, using a complete GI response outcome measure.
This is a common endpoint used in drug development for antiemetics and defines the complete responder as a patient who reaches the end of a study period without vomiting and without receiving a rescue antiemetic.
(09:57) The results of this analysis for oliceridine are extremely compelling. In the Phase III heart tissue study, patients on oliceridine were three times more likely to complete the study without vomiting and without needing a rescue antiemetic compared to patients on morphine.
We saw a similar pattern in the Phase III soft tissue study.
Importantly, these results held true when we control for differences in level of pain relief achieved. Put it different way, oliceridine doses that provided pain relief comparable to morphine had strikingly lower GI side effects.
In addition, the improvements in GI tolerability were not due to differences in pre-existing risk for nausea or vomiting among the treatment groups. We believe this data reinforces the overall GI tolerability data for oliceridine.
I'd now like to introduce Dr. Tim Beard, who is a practicing general surgeon and is the Chair of the Department of Surgery and Medical Director of Research at Summit Medical Group in Bend, Oregon. Tim also serves as an affiliate Professor of Surgery at Oregon Health Sciences University.
We've asked Tim to join us this morning to provide his perspective on the current clinical challenges he faces in his hospital and outpatient practice and his thoughts on the oliceridine data. Tim?
Timothy Beard (11:10)
Thank you, Mark, for the introduction. I'm pleased to join the Trevena team this morning to provide my perspective on the current role of IV opioid analgesics in my clinical practice and to share my thoughts on the body of data that the company has amassed on their investigational product, oliceridine.
I'm speaking on my own accord and not in my position as a general surgeon at the Summit Medical Group. I am a paid consultant with Trevena.
I practice as a general surgeon in a large multispecialty group and split my time between a community hospital and a physician-owned busy outpatient surgery center. I perform approximately 750 cases a year, with a third of those being done as inpatients.
I have spent a considerable amount of time reviewing the published data for this compound and I have assisted Trevena's R&D group in data analysis and participated as an author on some of the key publications.
I believe this experience has provided me some insights into what can be expected from oliceridine's potential use in practice.
While the role of IV opioids in the post-operative pain management has undergone an evolution over the years, these medications remain the pillar and standard of care for acute pain management.
In my practice, drugs such as IV morphine, dilaudid and fentanyl remain an integral part of all post-operative pain management strategies. The main reason for this is that only these medications can provide the definitive pain relief required in certain highly painful post-operative circumstances. I can't perform surgeries in my clinical practice without them.
Poorly managed pain can have many undesirable consequences, including a lack of mobility, poor appetite, and disrupted sleep patterns. On the flip side, drugs like IV morphine also have side effects including respiratory depression, ileus, nausea and vomiting.
So, you're left with a few options but to prescribe opioids when they're required, and then to supplement their use with several additional medications in order to try to minimize or counteract these side effects.
Because of this, I frequently find it necessary to prescribe as many as five to seven different additional drugs in the post-operative setting.
This unavoidable polypharmacy poses additional challenges to patients' recovery, including an increased risk of drug-drug interactions and the poor rate of adherence to these additional medications.
In my opinion, Trevena's investigational product oliceridine offers the first truly novel advance towards a solution to this problem.
I have been impressed with the quality and amount of data Trevena has gathered and published in peer-reviewed journals. The two pivotal Phase III studies provide the initial clinical data in bunionectomy and abdominoplasty surgeries. And these results showed great pain relief with a potentially differentiated and improved side effect profile from what we expect with conventional opioids.
The results from the Phase III or real world open label safety study extended these findings. Of particular interest to me was the diverse patient population of this study, many of them with multiple comorbidities, including older age, obesity and diabetes.
These types of high-risk patients represent ones I operate in my practice all the time. These complicating risk factors can pose significant challenges to a patient's post-operative course.
A recent patient I treated does come to mind. This was a 52-year-old woman who needed surgery for a near obstructing tumor in her distal transverse colon. And at the same time came to surgery with a history of poorly controlled diabetes and a BMI of 53.
The challenge here was not the surgical procedure itself, but the risks that emerged in her post-op recovery, given her high risk health history. For example, her surgical wound presented a huge infection risk. So, any occurrence of nausea, vomiting or retching could disrupt the integrity of her wound and lead to an infection.
This is just one example of the type of patient who I could potentially benefit from the profile that oliceridine appears to offer.
In his remarks, Mark noted the complete GI responder analysis from the clinical trials. Overall, these data suggests that, when the magnitude of analgesic benefit is held constant across treatment groups, patients treated with oliceridine are more likely to achieve a complete GI response compared to patients treated with morphine.
This is an important endpoint and I feel relevant to me when considering the management of the patient I just discussed. Decreasing the risk of vomiting by two or three fold might make the difference for this patient of having a relatively straightforward post-operative course versus the risk that I would be seeing her back in the operating room to repair her wound dehiscence.
I also see the potential advantage that oliceridine could provide in the outpatient setting. My ambulatory surgery center performs about 1,300 cases per month. One of our limiting factors in this setting is the availability of recovery room beds. If patients are delayed in the recovery, it prevents us from starting more cases.
By far the most common reason for prolonged recovery time are pain, nausea and vomiting. As a result, the recovery room nurses are hesitant to give too much opioid medications as that makes patients sleepy and they do not breathe as well. On the other hand, if they give too little, patients will have too much pain, which itself may contribute to increased rates of nausea and vomiting.
Oliceridine's pharmacokinetic profile offers several attributes that could provide advantages in the setting of care. For example, its rapid onset of analgesic effect makes it very easy for physicians to use. There also appears to be no need to adjust the dose for renal insufficiency, which again makes it easy on physicians. This is especially important in my practice as all the nephrologists in our town or in our group. Thus, I see a lot of renally-impaired patients.
Oliceridine also appears to have no active metabolites, which makes pain management in the short-term setting, like an ambulatory surgery center, more straightforward.
All of these factors could contribute to a decreased length of stay in our recovery room and increase patient satisfaction.
To sum up, I'm excited by the oliceridine data that I have seen, and I believe that oliceridine has the potential to help address some of the post-operative challenges that physicians and their patients still face.
Thank you again for the invitation to speak. And now, let me pass the call back to Mark.
Mark Demitrack (17:38)
Thanks, Tim, for your remarks. We greatly appreciate hearing your perspective on the challenges you face in your practice and what improvements you really hope to see in the current treatment landscape that would benefit both you and your patients. Tim will be available to answer questions during the Q&A later on this call.
I'd now like to turn the call over to Barry for a review of our full-year financials.
Barry Shin
Thanks, Mark. We issued our press release and filed our Form 10-K with our full financial results. For now, I'll summarize the headline numbers.
For the fourth quarter of 2019, we had a net loss of $6.4 million or $0.07 per share, compared to $8.0 million, or $0.10 per share, for the fourth quarter of 2018.
For the full-year 2019, we had a net loss of $24.9 million, or $0.27 per share, compared to $30.8 million, or $0.42 per share, for 2018. This decrease in net loss is mainly due to a headcount reduction in 2018 and a decrease in R&D expenses related to TRV250.
At year-end 2019, we had cash, cash equivalents and marketable securities of $35.8 million. With additional clarity following completion of our healthy volunteer study, I'm very happy to update our guidance and report that we expect this amount both under operations and capital expenditures into the first quarter of 2021.
This includes pre-commercial preparations and post-approval activities to ensure oliceridine will be available for distribution either by us or with a commercial partner in the fourth quarter of 2020. It also includes completion of a proof-of-concept study for TRV250 in acute migraine and IND-enabling work for TRV045.
We'll now open the call for questions, after which Carrie will provide some closing remarks.
Question-and-Answer Session
Operator
Thank you. [Operator Instructions]. The first question is from Jason Butler of JMP securities. Please go ahead.
Jason Butler (20:12)
Hi. Thanks for taking the questions. I had two for Dr. Beard. First of all, you talked about the types of patients that you might use for drug in. Can you talk about how you think about the procedures that you're doing and which procedures maybe warrant using the drug more than others? And then, can you just give us any thoughts you have on cost considerations of using a new drug like oliceridine and how those cost considerations compare and contrast in different institutions? For example, the community hospital you work in versus the outpatient clinic. Thanks.
Carrie Bourdow
Great. Thanks. Thanks, Jason. I actually think those are three questions, but, okay. Well, that'll be alright. So, Tim, I don't know if you could hear the first questions around the types of procedures in addition to the patients that you mentioned. And then secondly, talking a little bit more about cost, contrasting between the hospital and your ambulatory surgery center business.
Timothy Beard (21:25)
Sure. Well, the procedures, I kind of split them up into two different and then same with the costs. So, if you look at our inpatient, the procedures, I think, where oliceridine will be best are procedures that cause more pain. So, any sort of laparotomy where you're making big incisions, any sort of thoracotomy where you're going into the chest with, again, big incisions. We're trying our best to manage those with multimodal analgesia, but opioids play a key role. So, I would say any, again, procedure that causes a lot of pain, so maybe not as much minimally invasive, although I still see a role in minimally invasive surgery which is laparoscopic and robotically. I guess that would be for the inpatient.
And outpatient, what I'm excited for is the fact that this drug with what appears to be lower side effects that we'd be able to give people pain free and out of the recovery room faster. So, any patient I do in an outpatient surgery center, I think, there would be a role for this drug because, again, we are limited in space by recovery room. And if we get back up in the recovery room, everything kind of slows down.
So, I do the majority of my patient cases in an outpatient surgery center, to be honest with you, and that's the trend nationally as more and more stuff is being done as outpatients and a big part of that is controlling costs. So, I would say almost all patients we do as outpatients would be good candidates for this drug.
Now, costs are interesting. In the hospital, it would get absorbed in what's called the DRG. And the hospital looks at costs somewhat, but not super strict because it seems to me, like in our hospital, that DRG payments are fairly large, and they don't micromanage us very much on if we're using drugs that are a little bit more expensive than others. Sometimes, a little bit, we will get pushback. That's mostly on antibiotics. And that's mostly so you're not changing the form of antibiotics in our area.
In the outpatient surgery center, the margins on the cases are much smaller, and so costs are looked at more. So, I don't have any idea of what this drug is going to come out as cost-wise. But that would be looked at a little more as far as do we see a benefit from that.
But, again, I think most of us at the surgery center look at the bigger picture. So, if a drug does cost a little more, but people are happier getting out of the surgery center faster and we're more efficient, then the overall efficiency, I think, would far outweigh the cost of the drug.
An example of that is when IV Tylenol came out. That's a lot more expensive than oral Tylenol, but yet we use it quite a bit because we see a benefit with that drug, even though the cost is more.
So, I hope that answers your question.
Jason Butler (24:19)
That's great. Thank you very much. And thanks for taking the questions.
Carrie Bourdow
Thank you. Thanks, Jason.
Operator
The next question is from Douglas Tsao of H.C. Wainwright. Please go ahead.
Douglas Tsao (24:29)
Hi, good morning. I guess my first question is for Dr. Beard. In terms of you think about your overall patient population, both inpatient and outpatient, or you could address them separately, what percentage of them do you think fall into this high risk category and would be candidates for use once it is eventually hopefully approved?
Carrie Bourdow
Great. Thanks. Thanks, Doug. Great question. Dr. Beard, did you hear the questions, the percent of high-risk patients. Yeah?
Timothy Beard
Yeah. So, that percent goes up daily, it seems. I don't know. That was a real patient example that I gave. She was 5′1″, 325 pounds. So, that was an extremely difficult case and extremely difficult post-operative recovery. So, I would think, in our hospital, when this drug gets approved in August, we'd probably be able to get it to the P&T pretty fast, would be my guess.
And you probably start using it on higher risk patients. So, people with pulmonary issues, people that are at risk for nausea and vomiting. For example, I do a lot of laparoscopic foregut surgeries, which are called Nissen fundoplication or paraesophageal hernia repairs, mostly for heartburn and reflux, and if those patients retch or vomit, it can totally disrupt the wrap that you've done.
So, I would say, if I had to give a number of inpatients that I would say are what I would consider higher risk and that this drug is just tailor-made for, it'd put it probably at 50% or 60%. Unfortunately, I don't have a practice where I can operate on all this in healthy patients all the time, I wish. But this doesn't exist in reality.
Again, in the outpatient, these are healthier patients by definition. We don't do anyone over an ASA 3 in an outpatient surgery center, so they're healthier. But I think their benefit, again, it's a little different. It's not so much for their post-operative risk. The drug would be used for its what appears to be lower side effect profile and patient satisfaction and ease of getting them to our system.
Douglas Tsao (26:45)
And then, just one follow-up. Or two follow-ups, one for Dr. Beard. I know you mentioned you're often treating – sort of taking a polypharmacy approach. Just curious what drugs oliceridine alone would be able to replace. And then, just a question for Carrie in terms of TRV045, the S1P, which are going into epilepsy. Just curious, how it was epilepsy was the first indication selected for development? Thank you.
Carrie Bourdow
Great. Yeah. Tim, I'll let you start on oliceridine.
Timothy Beard (27:19)
Sure. So, we've developed these massive what are called ERAS pathways after surgery for a lot of our surgeries, which is Enhanced Recovery After Surgery. I'm sure you're familiar with them. And in that pathway, we do everything we can to optimize patients postoperatively. So, let's say I do a colectomy on someone, take out a colon for colon cancer. We obviously do a lot of stuff pre-op for those patients, but postoperatively even though they may get tap blocks or these rectus sheath blocks, they all get IV opioids. So, the drugs we give to counteract IV opioids, we give a drug called alvimopan or Entereg, which is a peripheral acting new opioid receptor antagonist, which blocks the side effects that opioids have on the gut. So, opioids cause an ileus where they cause the gut not to move. You can't pass gas or stool. So, you get that drug. We give a whole bevy of antiemetics, probably at least three different antiemetic to prevent the nausea and vomiting, including sometimes we give Decadron in surgery or Zofran or Phenergan or Compazine, any of those we can give to stop the post-operative nausea and vomiting.
We also then are super aggressive with our respiratory care on these patients. So, we get a respiratory therapy consult, do incentive spirometers and may or may not give them nebulizers if they need it. So, I think those are the three sort of main areas that we were giving drugs to counteract the side effects of opioids.
Carrie Bourdow
And it sounds like – it's difficult for you right now to say what oliceridine may replace. You've got to get it in your hands, I think, and use it, right, is really Doug's question around what potentially oliceridine could replace.
Timothy Beard
Right. We're hoping – because, yeah – and what I tried to mention in my talk is that when you give so many different drugs to the polypharmacy that the compliance to that regimen is fairly low. That's what we're finding out with our ERAS protocol, is that we give all these different drugs and then people actually don't really get them scheduled because it's too much, the compliance is fairly low. So, yeah, we don't know. That's why I'm excited for this drug to get approved to try it to see how much we can eliminate because anything we can do to simplify it would be great.
Carrie Bourdow (29:42)
Thank you. Thank you. And then, Doug, to follow-up on your question on S1P, so quick reminder, and I'll turn it over to Mark to talk specifically about epilepsy, but there are other areas that we've studied with TRV045 or in the process of looking at. Chemo-induced peripheral neuropathy is another area that we've looked at on the animal data. And then, epilepsy was really – Mark is going out and talking to folks that are involved in looking at epilepsy drugs and epilepsy trials. So, Mark, I'll let you talk a little bit about…
Mark Demitrack (30:18)
Doug, it's a great question. And as you know, we've talked in the past, the S1P target is really quite interesting because of its broad representation in the CNS. So, really, the challenge for us is more focused since there's an enormous number of targets that are of potential interest.
And as Carrie mentioned, most of our early work was focused on chemotherapy-induced peripheral neuropathy in rodent models. That's one of the best studied animal models for the S1P system. But because of S1P localization on cell types in the brain, particularly glial cell types or astrocytes, it has demonstrable impact on various measures of membrane stability. And as a result, people became interested in the idea of exploring it in epilepsy models. And although it's not as well studied as the CIPN work, there has been some animal work done with some of the available S1P ligands, like fingolimod, for example. Now, you know that fingolimod is a non-selective S1P modulator and it also is accompanied by peripheral immunosuppression.
The S1P1 receptor target, which is what 045 is directed at, is a bit more selective to the CNS receptors and it also is absent in immunosuppression in our studies to date. So, it allows us to build on some of the literature that exists for the epilepsy target in animal models with earlier tool compounds. And that really is kind of the thing that prompted our interest.
The collaboration with EPSP emerged from those discussions. EPSP program is a longstanding, well regarded preclinical screening program that's sponsored by NINDS through the NIH. It's been in existence for about 30 years and has actually shepherded along several pretty key anti-epileptics to the market in their experience. So, we're pretty gratified that in our discussions that we've engaged in this program. So, further updates in the future.
Carrie Bourdow
Thank you. Thanks. Great.
Operator
This concludes the question-and-answer session. I would now like to turn it back to Carrie Bourdow for closing comments.
Carrie Bourdow
Great, thank you. And thank you for your questions. Thank you to Dr. Beard for addressing the questions. We appreciate that.
Let me close with some of the key points that you heard today. First, we've executed on our plan. We did what we said we were going to do. We resubmitted the NDA for oliceridine, got confirmation from FDA that the submission was complete, and we also advanced the pipeline, as we carefully managed our expenses.
I'd like to add my thanks to the team for their hard work and commitment. We expect 2020 to be a transformational year for Trevena. With the oliceridine NDA now under FDA review, we're preparing for expected approval in August. And we're also going to continue to make progress on the pipeline. So, I will continue to provide updates as the year progresses. Thank you again for joining us this morning on the call.
Operator
This concludes today's teleconference. You may disconnect your lines at this time. Thank you for your participation.
I recommend listening to the actual call (24 minutes, 54 seconds). Go to Trevena to register and to listen:
https://www.trevena.com/investors/press-releases/detail/228/trevena-reports-fourth-quarter-and-full-year-2019-results
Trevena, Inc. (NASDAQ:TRVN) Q1 2020 Earnings Conference Call May 7, 2020 8:00 AM ET
Company Participants
Robert Yoder - Senior Vice President and Chief Business Officer
Carrie Bourdow - President and Chief Executive Officer
Mark Demitrack - Senior Vice President and Chief Medical Officer
Barry Shin - Senior Vice President and Chief Financial Officer
Conference Call Participants
Jason Butler - JMP Securities
Douglas Tsao - H.C. Wainwright & Co., LLC
Operator
Ladies and gentlemen, thank you for standing by, and welcome to the Trevena, Inc. First Quarter Earnings Conference Call. At this time, all participants are in a listen-only mode. After the speaker presentation, there will be a question-and-answer session. [Operator Instructions] Please be advised that today’s conference is being recorded. [Operator Instructions]
I would now like to hand the conference over to your speaker today, Mr. Bob Yoder, Chief Business Officer. Thank you. Please go ahead, sir.
Robert Yoder
Good morning, and welcome, everyone. Thank you for joining us on this morning's call. With me today are Carrie Bourdow, our President and CEO; Mark Demitrack, our Chief Medical Officer; and Barry Shin, our Chief Financial Officer.
Before we begin, we wish to inform participants that we will be making forward-looking statements on this call, which are made pursuant to the safe harbor provision of the Private Securities Litigation Reform Act of 1995.
You are cautioned that forward-looking statements involve risks and uncertainties, including risks detailed from time-to-time in the Company's periodic reports filed with the Securities and Exchange Commission, and we undertake no obligation to update these statements beyond today.
During today's call, Carrie will give some opening remarks on our progress of oliceridine and I'll provide an overview of our commercial launch strategy. Mark will then provide some additional details on our ongoing pipeline activities and Barry will review our financial results followed by some time for questions.
I'll now turn the call over to Carrie.
Carrie Bourdow
Thank you, Bob. Good morning, everyone. Thank you for joining us today. I hope that you and your families are staying safe during these unprecedented and challenging times. I would like to open the call this morning by extending my many thanks to the healthcare professionals, our employees, and our business partners who help us move forward in our commitment to patients.
Like a lot of you, we are watching the COVID situation closely and while our priority of course is on the health and safety of our employees and our communities, I am also very grateful that we've been able to remain resilient and focused on business continuity.
And to that end, let me provide a few highlights on our lead asset IV oliceridine. As you all know, we have a PDUFA date for oliceridine of August 7, and it's clear to us that the agency is active in the review of our resubmission. I am very pleased with FDA's engagement, and we expect FDA's review of our application to continue on track. We are looking forward to receiving their decision in August.
At the same time, we are working to ensure that after approval and DEA scheduling, we can make oliceridine available to hospitals and healthcare providers in the fourth quarter of this year. Our commercial manufacturing facilities, which are located in the U.S. are manufacturing drug product as we speak.
We are also actively investigating collaborations and strategic partnerships to support the U.S. commercial launch of oliceridine and our current ex-U.S. partners are making progress on their regulatory timelines. Our top priority is getting oliceridine to acute pain patients and we are exploring all options to help us maximize shareholder value as we do this.
So now let me turn the call over to Bob, who will go into more detail on our U.S. commercial strategy. Bob?
Robert Yoder
Thank you, Carrie. Well, this is certainly an exciting time for us as we continue preparations for the commercial launch of oliceridine, either by ourselves or with a partner. As you'll hear me layout, our strategy is built around focus and efficiency, targeting the right patient population, physician specialties and accounts in order to facilitate initial uptake.
The market opportunity is large with approximately 45 million patients each year who receive drugs like IV morphine for acute pain. Additionally, the overall size of the market in terms of unit sold has remained relatively stable over the last 18 months, suggesting that potent analgesics such as IV morphine are still needed in the hospital settings.
The product profile oliceridine when compared to IV morphine, it's differentiated in a number of key areas. Unlike morphine, oliceridine has a fast onset of two to five minutes, no known active metabolites and no dosage adjustment needed in elderly or renally impaired patient.
Oliceridine offers a compelling set of attributes that address the unmet needs that still remain to both the inpatient and outpatient settings. We know that roughly 20% of the overall hospital patient population are considered high-risk for adverse effects, including patients with certain comorbidities, obese patients, those with renal impairment and the elderly.
We refer to this subset as our core patients. Physicians continue to face particular challenges in effectively and safely treating these patients and those challenges have unfortunately been highlighted by the ongoing pandemic.
In ATHENA, our open-label, real world safety study published last year, we studied many of these high-risk patients across a range of surgical settings. In fact, 30% of patients were over the age of 65 and 50% were clinically obese.
You may recall during our last earnings call in March, Dr. Tim Beard, a colorectal surgeon practicing in Oregon described patient types very similar to those we study, who he felt might benefit from a drug such as oliceridine.
Our launch strategy is focused and targeted. The core patients I described earlier will be our initial focus as those patients currently present the greatest difficulty in pain management. We also plan to concentrate initially on a subset of physician specialties, anesthesiologist, colorectal, orthopedic, and cardiothoracic surgeons.
These specialties have a high volume of procedures in which multimodal pain management, protocols frequently required drugs such as IV morphine. These facilities are also treating a high number of our core or high-risk patients. Finally, we plan to focus on a subset of hospitals and outpatient surgery centers that have demonstrated early adoption of other branded agents in the past.
Of course, we are closely monitoring the impact of the current pandemic and how that could change our thinking about our commercialization strategy. But we continue to hear about high-risk patients, the challenges these patients present in effective pain management and growing pent-up demand created by pauses and procedures considered to be elective surgeries and exacerbated by the current shortage of drugs like IV morphine.
In closing, we are taking an approach to commercialization that is all about focus. The right group of patients treated by a targeted subset of physician specialties and within a group of hospitals and surgery centers where we believe the potential oliceridine is significant.
Let me now turn the call over to Mark to provide some additional details on our pipeline activities.
Mark Demitrack
Thank you, Bob. Let me start with some additional comments on oliceridine. I am pleased to report that we've continued to add to the body of peer-reviewed literature, which is an important element supporting the launch strategy that Bob just outlined.
We recently announced the publication of a comprehensive review of the non-clinical and clinical data for oliceridine. In addition, I would like to highlight the online publication of a poster in association with this year's ASRA meeting.
The poster is titled Low Incidence of Opioid-Induced Respiratory Depression in High-Risk Elderly Obese Patients. This report summarizes the findings of a post-hoc analysis of data from an ATHENA study. We compared the incidence of clinical indices of respiratory depression across two patient subpopulations in that study.
Those considered high-risk and those considered low-risk. High-risk patients were those individuals who were over 65 years old and had a BMI greater than 30. As Bob mentioned earlier, these patients were a large proportion of the study population. Low-risk patients were defined as the opposite, those younger than 65 with a BMI less than 30. The results were very interesting to us.
The incidence of respiratory depression was similar in both groups, despite the high-risk group being defined by two characteristics known to raise the risk of respiratory complications during treatment with conventional medications like IV morphine.
These data are consistent with feedback we received from investigators during the ATHENA study on their assessment of oliceridine's distinctive clinical profile. These data will serve as an important point of departure for our thinking about future research.
Beyond oliceridine, we continue to make good progress with our pipeline for TRV045, our novel S1P receptor modulator. Our collaboration with NIH is ongoing and productive. They've initiated the first round of non-clinical studies in their epilepsy screening program and we look forward to reporting on that work in the future.
Most of us announced this morning that NIH plans to begin evaluating TRV045 within another screening program. This one designed to study novel non-addictive treatments for pain. This program is based on the longstanding epilepsy screening program, which is viewed as a highly successful partnership model and also features a rigorous evaluation process for entry.
The program includes assays and models of acute, inflammatory and neuropathic pain, all of which were funded by NIH. The fact that TRV045 has received such interest from NIH, I believe speaks to its exciting promise as a novel approach to treating a variety of CNS disorders.
I look forward to working closely with NIH to further explore the therapeutic potential of this asset. In parallel with these activities, we continue to make progress on our own IND-enabling work with this compound, and I am very pleased to announce that we are now planning on filing an IND application for TRV045 in the first half of 2021.
I'd now like to turn it over to Barry for review of our Q1 financials. Barry?
Barry Shin
Thanks, Mark. We issued a press release. We filed our Form 10-Q with our full financial results. For now, I'll summarize the headline numbers. For the first quarter of 2020, we had a net loss of $5.7 million or $0.06 per share, compared to $5.2 million or $0.06 per share for the first quarter of 2019. This increase in net loss is mainly due to higher R&D expenses associated with a TRV250 acute migraine proof-of-concept study and activities to support the NDA resubmission for oliceridine.
As of March 31, 2020, we had cash and cash equivalent of $28.1 million, which reflects the full repayment of our term loan on March 2. We continue to expect that this amount will fund our operations and capital expenditures into the first quarter of 2021. This includes the expected approval of oliceridine in August and post-approval activities to ensure oliceridine as commercially available in the fourth quarter of 2020.
We'll now open the call for questions, after which Carrie will provide some closing remarks. Rachel?
Question-and-Answer Session
Operator
[Operator Instructions] Your first question comes from the line of Jason Butler. You may begin.
Jason Butler
Thanks for taking the questions. First one on oliceridine, can you just give us any color around manufacturing inspection? Did you have a pre-approval inspection during the first cycle NDA review? And do you expect that any additional inspections to be needed by FDA before your PDUFA date?
Carrie Bourdow
Good morning, Jason. Thanks for the question. We did not have previously an inspection, but the – so I mentioned the sites are in the U.S., the API and drug product sites are in the U.S., which we think is a good thing. And they have been inspected last year for other products, didn't have any issues, no 483, so we're not anticipating manufacturing is going to be a problem at all for us.
Jason Butler
Okay. Great. You ran through some of the patients you're targeting – the high-risk of adverse events and the physicians as well. As you think about the beginning of a resumption of elective procedures, where is the overlap and how do you think about the dynamics of which procedures could ramp sooner and where we could see a prolonged proponent procedures and ultimately are you looking to refocus any of your launch strategy in response to these dynamics? Thanks.
Carrie Bourdow
Yes. So I'll let Bob address this. But let me just say that we're talking with a lot of our key opinion leaders across the country and it's not necessarily, which procedures may start kicking in sooner. It's really based on geography in some cases.
Our core areas, as Bob mentioned, cardiothoracic, colorectal, orthopedic, certainly cardiothoracic, we believe will start happening sooner, and of course, like everyone are sort of thinking through what our launch strategy will look like.
Let me just brag on Bob really quickly before I turn it over. So one of the reasons we asked Bob to join Trevena is that he has a lot of experience in non-personal promotion launches, launching with more of a digital focus. I think that's going to serve us well when we sort of think through our launch strategy. But Bob, any additional comments?
Robert Yoder
Sure, yes. Hi, Jason. Thanks for the question. So one thing I'd say about the procedures piece of it, is the things I'm reading at least say as an elective procedures that were paused or canceled or coming back online.
What I've been reading is that the patient type that they're looking to prioritize are typically those higher risk patients because often times that profile just gets riskier with time. So they're trying to in many cases push those high-risk patients to the front of the queue as those procedures come back.
Around the strategies, obviously we're watching very closely what the pandemic is doing to HCP engagement. In this case, I think the early trends seem to suggest that physicians are engaging remotely a little more. They're open to that more. Digital channels are getting more robust as well.
So I think, overall, an effective engagement on the future of what we're going to be thinking about is likely, the flexibility to dial up or dial back a wider array of channels, digital channels, non-personal promotion and things like that. Certainly, until we see what will happen with traditional face-to-face access with HCPs over time. But definitely we're going to keep an eye out and think creatively about how we're going to engage with HCPs and what – I guess will be the new normal going forward.
Jason Butler
Great. And then just one more for me on 045, obviously the work being done at NIH, can you discuss or point to any additional preclinical work that you guys need to do in-house to support the IND filing in the first half of next year? Thanks.
Carrie Bourdow
Yes. Thanks, Jason. Mark, you want to talk a little bit about…
Mark Demitrack
Sure, Jason. So our [indiscernible] activity really revolves around much of the conventional components with any IND that we need to be assembled. So we have to obviously proceed with the necessary tax work and the manufacturing readiness that we needed for the formulation that we would bring into human use. So those programs are proceeding as I mentioned on plan at this time.
Jason Butler
Okay. Great. Thanks for taking the questions.
Carrie Bourdow
Thanks, Jason. Any other questions operator? Rachel?
Operator
Your next question comes from the line of Douglas Tsao. You may ask your question.
Carrie Bourdow
Good morning, Doug.
Douglas Tsao
Good morning. Just you maybe first touch on a little bit and obviously you've spoken about sort of some of the delays and sort of the backlog and intellective procedures, just sort of the context of the shortages that seem to be taking place for a lot of IV pain medications, just given the demand placed on hospitals because of COVID, and does that affect your launch strategy in anyway? And then also and I might have missed it, a lot going on in the household this morning.
Carrie Bourdow
Yes.
Douglas Tsao
Just in terms of the pause for TRV250 and when you might be able to get that started again?
Carrie Bourdow
Yes. So let me handle that first and then I'll turn the question over to Bob around some of our additional commercial strategy. So on TRV250, as you mentioned, we are on pause. That study is being conducted in the UK. And like everyone, we're sort of watching and having conversations with the clinical site in the UK.
So as soon as they feel comfortable to get moving again, we'll be doing that, but we don't have any additional guidance on that. We removed the timing guidance on TRV250. But we are having active conversations with the clinical site. So it's good.
Bob, do you want to – I know you talked a little bit about the commercial strategy in COVID and COVID patients, but any other additional comments you want to make certainly with the focus around high-risk patients in COVID? We've always been focused in high-risk patients, but there's a heightened sensitivity of what happens when those patients get sick in the hospital. So I don't know if you want to talk a little bit more about that.
Robert Yoder
Yes. Hi, Doug. I mean, I think you're right. You're pointing out definitely that's the – there's many unfortunate things around the pandemic and certainly one of them is [indiscernible]. We've all seen now that these high-risk patients present a lot of challenges in clinical management.
Specific to your question around the shortage too, I mean, I think, there is some data out there publicly [indiscernible] talked about at least within March, maybe the first part of April even that there is a pretty significant shortage. I think fill rates were hovering in the 70% range for IV opioids-driven. I think a lot I use in COVID patients, incubated patients. But the other impact of that is that that leaves – that’s available for use in post-surgical moderate to acute pain – moderate to severe pain.
So I mean, I think, I don't know beyond what I said before Doug in terms of change of strategies, it certainly tightens our urgency to be prepared for a really successful launch and get the product out there. So that compelling profile is in the hands of our physicians and they can use it where it's indicated, where they see fit.
Douglas Tsao
And maybe as a follow-up, I know it's still obviously very early days, and you're sort of limited in what you can do in terms of gauging with clinicians at this point. But just curious if you've gotten feedback from people sort of anxious to get it, because obviously I think the COVID-19 crisis has really sort of exposed the vulnerability of the American Healthcare System from a capacity standpoint.
Are you getting feedback that sort of greater interest in oliceridine because that's certainly one of the attributes of the product is really to sort of help improve efficiency of the system, which perhaps I think we probably took for granted before this sort of took place.
Carrie Bourdow
Yes. It's a really good point. I mean, I think we've talked before about the – in particular the investigators that were involved in ATHENA are interested in getting oliceridine, having oliceridine has an alternative. We're three months away from PDUFA date. So I think that's – they're excited about that potential opportunity of having oliceridine here relatively soon.
I do agree with you. I think, as I mentioned earlier, in particular the high-risk patients, right. Well we've talked about, you've heard us talk about is when these patients get sick, they stay even longer in the hospital. They put a lot of cost into the hospital system, some of the hardest, most difficult patients to treat.
So it's been a focus of ours since the beginning to focus on those patients. That's where we think we'll get the initial use for oliceridine. Beyond that, as it relates to COVID, I think we're all sort of watching things and staying focused on getting oliceridine approved by the agency.
Douglas Tsao
Okay. Great. That's it for me. Thank you.
Carrie Bourdow
Thank you, Doug. Appreciate it.
Operator
I am showing no further questions at this time. I would now like to turn the conference back to Carrie Bourdow, CEO.
Carrie Bourdow
Great. Well, thank you all. I appreciate all of the questions this morning. And as you can hear, we are optimistic and excited about oliceridine and PDUFA date that is quickly coming up. We are also excited about TRV045 and the NIH interest in 045 and also the progress that we've made in our IND capabilities and the ability to have an IND hopefully in the first half of next year.
So thank you again for the time despite all the craziness that we're all dealing with. As you hear, we are passionate about our mission in developing novel medicines for patients in need. Thank you again for joining us this morning.
Operator
Ladies and gentlemen, this concludes today's conference call. Thank you for participating. You may now disconnect.
Q4 2019 Results Earnings
Conference Call March 12, 2020 8:00 AM ET
I recommend listening to the actual call (33 minutes, 59 seconds). Go to Trevena to register and to listen: https://www.trevena.com/investors/press-releases/detail/228/trevena-reports-fourth-quarter-and-full-year-2019-results
Trevena, Inc. (NASDAQ:TRVN) Q4 2019 Results Earnings Conference Call March 12, 2020 8:00 AM ET
Company Participants
Robert Yoder - Senior Vice President, Chief Business Officer
Carrie Bourdow - President and Chief Executive Officer
Mark Demitrack - Senior Vice President, Chief Medical Officer
Timothy Beard - Chair of the Department of Surgery, Summit Medical Group
Barry Shin - Senior Vice President, Chief Financial Officer
Conference Call Participants
Jason Butler - JMP Securities
Douglas Tsao - H.C. Wainwright & Co.
Operator
Greetings and welcome to the Trevena Fourth Quarter and Full-Year 2019 Earnings Call. At this time, all participants are in a listen-only mode. A brief question-and-answer session will follow the formal presentation. [Operator Instructions]. As a reminder, this conference is being recorded.
It is now my pleasure to introduce your host, Bob Yoder, Chief Business Officer. Please go ahead.
Robert Yoder (00:30)
Thank you and welcome, everyone. Thank you for joining us on this morning's call. With me today are Carrie Bourdow, our President and CEO; Mark Demitrack, our Chief Medical Officer; Barry Shin, our Chief Financial Officer; and Timothy Beard, Chair of the Department of Surgery at Summit Medical Group in Bend, Oregon.
Before we begin, we wish to inform participants that we will be making forward-looking statements on this call, which are made pursuant to the Safe Harbor provision of the Private Securities Litigation Reform Act of 1995. You're cautioned that such forward-looking statements involve risks and uncertainties, including risks detailed from time-to-time in the company's periodic reports filed with the Securities and Exchange Commission. And we undertake no obligation to update these statements beyond today.
During today's call, Carrie will review our 2019 and recent corporate achievements and lay out our plan for 2020. Mark will provide an overview of the data from our IV oliceridine program that was recently resubmitted to FDA. Dr. Beard has also joined us this morning to provide his perspective on the current role of IV opioid analgesics in his clinical practice. Barry will then review our financial results, followed by some time for questions.
I'll now turn the call over to Carrie.
Carrie Bourdow (01:43)
Thanks, Bob. Good morning, everyone. Thank you for joining us this morning. At the start of 2019, you'll remember that I laid out a plan to resubmit oliceridine for approval and to advance the pipeline.
What you're going to hear this morning on this call is that we've delivered on the plan and you'll hear that with successful resubmission of oliceridine, we'll now turn our attention to preparing for expected approval in August of this year.
And on the pipeline front, what you'll hear is that we've hit key development milestones. We now have two proof-of-concept studies underway – one for acute migraine and another for opioid use disorder. And we're studying TRV045, a novel S1P modulator in epilepsy and a variety of other CNS conditions.
Importantly, we completed all of this work while we managed our expenses very carefully. And I have to say I am extremely proud of this team and what was accomplished in 2019.
Let me give you just a few more details on the highlights, the high points from my perspective from the year. As you saw last week, FDA accepted our resubmission of the oliceridine NDA and it's crazy. They told us that it was a complete response to their action letter. They set a PDUFA date of August 7 and we're looking forward to working with them as they review our application.
In the past, you've heard me talk about the market opportunity for oliceridine. It's large. Over 45 million patients each year in US hospitals receive drugs like IV morphine for acute pain, and about 9 million of those patients are at greater risk of developing adverse events. Hospitals are seeing a rise in these at-risk patients and an increase in the number of severe acute pain surgery.
And we believe this at risk patient population alone represents a total addressable market of $1 billion to $1.5 billion. That's impressive.
But at the end of the day, it's important that we focus on why we developed a novel analgesic like oliceridine and the reason is to improve patients' lives. Later on this call, we've invited Dr. Tim Beard to talk with you about some of his high-risk patients and the challenges that he faces in managing post-op acute pain.
Beyond oliceridine, we made significant progress on the pipeline. Late last year, we initiated an acute migraine proof-of-concept study for TRV250. Migraine is also another large market. Approximately 650 million migraines are treated annually in the US. And there's still a need for novel treatment options.
TRV250 is a novel new mechanism, and this one at the delta receptor. And the delta receptor is located throughout the brain and the delta receptors regulate mood, anxiety and pain, including migraine pain. We're evaluating the ability of TRV250 to reduce the occurrence of headaches and also to potentially reduce symptomatic anxiety. About half of all migraine patients experience anxiety.
There are no approved treatment options that can treat both migraines and anxiety. So, obviously, this would be a large market opportunity for us for TRV250. It's a really exciting asset and we're expecting top line results on this study in the second half of this year.
Another proof-of-concept study we started late last year was in collaboration with the National Institute on Drug Abuse, or a group called NIDA. And this study is for TRV734 for opioid use disorder.
NIDA is looking at the potential of 734 as a safer and better tolerated treatment option for patients suffering from addiction. We're really pleased to be working with NIDA to help fight the opioid crisis and I'll keep you updated as the study progresses.
And then lastly, as you saw this morning, we announced that we've initiated another collaboration with the NIH to investigate the potential of TRV045 as a treatment for epilepsy. 045, another new mechanism, represents a novel approach to treating neurological disorders. And it's a next generation S1P receptor modulator that activates the receptor target without any of the immunosuppression that you get with other S1P modulators.
NIH has already initiated the first round of assays for epilepsy. And we believe this asset holds promise not only for epilepsy, but for a variety of CNS indications.
With all of our assets, including oliceridine, we're actively investigating collaborations and strategic partnerships. Remember, we already have two ex-US partnerships for oliceridine. And these collaborations are going really well. We're expecting to receive a $3 million milestone payment upon FDA approval of oliceridine.
As we continue to make progress on oliceridine and the pipeline, we're going to continue to look for ways to advance all of our assets and to maximize shareholder value.
With that, let me now turn the call over to Mark.
Mark Demitrack (07:12)
Thank you, Carrie. I'm also very pleased that we've successfully re-submitted our NDA for IV oliceridine. This milestone represents more than a year of work by members of our clinical, non-clinical, manufacturing and regulatory teams. And I'm extremely grateful for the opportunity to work with such a dedicated group of individuals.
I believe the outcome of that work is compelling and further strengthens our evidence in support of oliceridine as a potential new treatment option for patients with moderate to severe acute pain.
The promise of oliceridine as a distinctive addition to a clinician's armamentarium of IV analgesics is built on its novel mechanism of action and unique pharmacokinetic profile.
Oliceridine is a new chemical entity, a first in this space in decades, and was designed to optimize G protein coupled receptor pharmacology by preferentially engaging the G protein signaling pathway responsible for analgesia, with reduced recruitment of beta-arrestin, which is largely involved in development of adverse effects.
Oliceridine has a rapid onset of action, with perceptible pain relief as early as two to five minutes after the first dose and lasting approximately three hours, providing a highly differentiated analgesic profile for clinicians.
Oliceridine also has no evidence of active metabolites, which can complicate dosing and result in the emergence of delayed adverse events.
Finally, our recently published studies in special populations have shown that no dosage adjustment is necessary in patients with underlying renal impairment or in the elderly. These attributes distinguish oliceridine from currently available IV analgesics like morphine.
As a reminder, we've amassed a comprehensive clinical data set for oliceridine across multiple efficacy and safety studies, involving over 1,800 individuals.
On past calls, we've spoken about the respiratory safety data, but today I'd like to highlight the GI tolerability data collected during our pivotal Phase III studies, using a complete GI response outcome measure.
This is a common endpoint used in drug development for antiemetics and defines the complete responder as a patient who reaches the end of a study period without vomiting and without receiving a rescue antiemetic.
(09:57) The results of this analysis for oliceridine are extremely compelling. In the Phase III heart tissue study, patients on oliceridine were three times more likely to complete the study without vomiting and without needing a rescue antiemetic compared to patients on morphine.
We saw a similar pattern in the Phase III soft tissue study.
Importantly, these results held true when we control for differences in level of pain relief achieved. Put it different way, oliceridine doses that provided pain relief comparable to morphine had strikingly lower GI side effects.
In addition, the improvements in GI tolerability were not due to differences in pre-existing risk for nausea or vomiting among the treatment groups. We believe this data reinforces the overall GI tolerability data for oliceridine.
I'd now like to introduce Dr. Tim Beard, who is a practicing general surgeon and is the Chair of the Department of Surgery and Medical Director of Research at Summit Medical Group in Bend, Oregon. Tim also serves as an affiliate Professor of Surgery at Oregon Health Sciences University.
We've asked Tim to join us this morning to provide his perspective on the current clinical challenges he faces in his hospital and outpatient practice and his thoughts on the oliceridine data. Tim?
Timothy Beard (11:10)
Thank you, Mark, for the introduction. I'm pleased to join the Trevena team this morning to provide my perspective on the current role of IV opioid analgesics in my clinical practice and to share my thoughts on the body of data that the company has amassed on their investigational product, oliceridine.
I'm speaking on my own accord and not in my position as a general surgeon at the Summit Medical Group. I am a paid consultant with Trevena.
I practice as a general surgeon in a large multispecialty group and split my time between a community hospital and a physician-owned busy outpatient surgery center. I perform approximately 750 cases a year, with a third of those being done as inpatients.
I have spent a considerable amount of time reviewing the published data for this compound and I have assisted Trevena's R&D group in data analysis and participated as an author on some of the key publications.
I believe this experience has provided me some insights into what can be expected from oliceridine's potential use in practice.
While the role of IV opioids in the post-operative pain management has undergone an evolution over the years, these medications remain the pillar and standard of care for acute pain management.
In my practice, drugs such as IV morphine, dilaudid and fentanyl remain an integral part of all post-operative pain management strategies. The main reason for this is that only these medications can provide the definitive pain relief required in certain highly painful post-operative circumstances. I can't perform surgeries in my clinical practice without them.
Poorly managed pain can have many undesirable consequences, including a lack of mobility, poor appetite, and disrupted sleep patterns. On the flip side, drugs like IV morphine also have side effects including respiratory depression, ileus, nausea and vomiting.
So, you're left with a few options but to prescribe opioids when they're required, and then to supplement their use with several additional medications in order to try to minimize or counteract these side effects.
Because of this, I frequently find it necessary to prescribe as many as five to seven different additional drugs in the post-operative setting.
This unavoidable polypharmacy poses additional challenges to patients' recovery, including an increased risk of drug-drug interactions and the poor rate of adherence to these additional medications.
In my opinion, Trevena's investigational product oliceridine offers the first truly novel advance towards a solution to this problem.
I have been impressed with the quality and amount of data Trevena has gathered and published in peer-reviewed journals. The two pivotal Phase III studies provide the initial clinical data in bunionectomy and abdominoplasty surgeries. And these results showed great pain relief with a potentially differentiated and improved side effect profile from what we expect with conventional opioids.
The results from the Phase III or real world open label safety study extended these findings. Of particular interest to me was the diverse patient population of this study, many of them with multiple comorbidities, including older age, obesity and diabetes.
These types of high-risk patients represent ones I operate in my practice all the time. These complicating risk factors can pose significant challenges to a patient's post-operative course.
A recent patient I treated does come to mind. This was a 52-year-old woman who needed surgery for a near obstructing tumor in her distal transverse colon. And at the same time came to surgery with a history of poorly controlled diabetes and a BMI of 53.
The challenge here was not the surgical procedure itself, but the risks that emerged in her post-op recovery, given her high risk health history. For example, her surgical wound presented a huge infection risk. So, any occurrence of nausea, vomiting or retching could disrupt the integrity of her wound and lead to an infection.
This is just one example of the type of patient who I could potentially benefit from the profile that oliceridine appears to offer.
In his remarks, Mark noted the complete GI responder analysis from the clinical trials. Overall, these data suggests that, when the magnitude of analgesic benefit is held constant across treatment groups, patients treated with oliceridine are more likely to achieve a complete GI response compared to patients treated with morphine.
This is an important endpoint and I feel relevant to me when considering the management of the patient I just discussed. Decreasing the risk of vomiting by two or three fold might make the difference for this patient of having a relatively straightforward post-operative course versus the risk that I would be seeing her back in the operating room to repair her wound dehiscence.
I also see the potential advantage that oliceridine could provide in the outpatient setting. My ambulatory surgery center performs about 1,300 cases per month. One of our limiting factors in this setting is the availability of recovery room beds. If patients are delayed in the recovery, it prevents us from starting more cases.
By far the most common reason for prolonged recovery time are pain, nausea and vomiting. As a result, the recovery room nurses are hesitant to give too much opioid medications as that makes patients sleepy and they do not breathe as well. On the other hand, if they give too little, patients will have too much pain, which itself may contribute to increased rates of nausea and vomiting.
Oliceridine's pharmacokinetic profile offers several attributes that could provide advantages in the setting of care. For example, its rapid onset of analgesic effect makes it very easy for physicians to use. There also appears to be no need to adjust the dose for renal insufficiency, which again makes it easy on physicians. This is especially important in my practice as all the nephrologists in our town or in our group. Thus, I see a lot of renally-impaired patients.
Oliceridine also appears to have no active metabolites, which makes pain management in the short-term setting, like an ambulatory surgery center, more straightforward.
All of these factors could contribute to a decreased length of stay in our recovery room and increase patient satisfaction.
To sum up, I'm excited by the oliceridine data that I have seen, and I believe that oliceridine has the potential to help address some of the post-operative challenges that physicians and their patients still face.
Thank you again for the invitation to speak. And now, let me pass the call back to Mark.
Mark Demitrack (17:38)
Thanks, Tim, for your remarks. We greatly appreciate hearing your perspective on the challenges you face in your practice and what improvements you really hope to see in the current treatment landscape that would benefit both you and your patients. Tim will be available to answer questions during the Q&A later on this call.
I'd now like to turn the call over to Barry for a review of our full-year financials.
Barry Shin
Thanks, Mark. We issued our press release and filed our Form 10-K with our full financial results. For now, I'll summarize the headline numbers.
For the fourth quarter of 2019, we had a net loss of $6.4 million or $0.07 per share, compared to $8.0 million, or $0.10 per share, for the fourth quarter of 2018.
For the full-year 2019, we had a net loss of $24.9 million, or $0.27 per share, compared to $30.8 million, or $0.42 per share, for 2018. This decrease in net loss is mainly due to a headcount reduction in 2018 and a decrease in R&D expenses related to TRV250.
At year-end 2019, we had cash, cash equivalents and marketable securities of $35.8 million. With additional clarity following completion of our healthy volunteer study, I'm very happy to update our guidance and report that we expect this amount both under operations and capital expenditures into the first quarter of 2021.
This includes pre-commercial preparations and post-approval activities to ensure oliceridine will be available for distribution either by us or with a commercial partner in the fourth quarter of 2020. It also includes completion of a proof-of-concept study for TRV250 in acute migraine and IND-enabling work for TRV045.
We'll now open the call for questions, after which Carrie will provide some closing remarks.
Question-and-Answer Session
Operator
Thank you. [Operator Instructions]. The first question is from Jason Butler of JMP securities. Please go ahead.
Jason Butler (20:12)
Hi. Thanks for taking the questions. I had two for Dr. Beard. First of all, you talked about the types of patients that you might use for drug in. Can you talk about how you think about the procedures that you're doing and which procedures maybe warrant using the drug more than others? And then, can you just give us any thoughts you have on cost considerations of using a new drug like oliceridine and how those cost considerations compare and contrast in different institutions? For example, the community hospital you work in versus the outpatient clinic. Thanks.
Carrie Bourdow
Great. Thanks. Thanks, Jason. I actually think those are three questions, but, okay. Well, that'll be alright. So, Tim, I don't know if you could hear the first questions around the types of procedures in addition to the patients that you mentioned. And then secondly, talking a little bit more about cost, contrasting between the hospital and your ambulatory surgery center business.
Timothy Beard (21:25)
Sure. Well, the procedures, I kind of split them up into two different and then same with the costs. So, if you look at our inpatient, the procedures, I think, where oliceridine will be best are procedures that cause more pain. So, any sort of laparotomy where you're making big incisions, any sort of thoracotomy where you're going into the chest with, again, big incisions. We're trying our best to manage those with multimodal analgesia, but opioids play a key role. So, I would say any, again, procedure that causes a lot of pain, so maybe not as much minimally invasive, although I still see a role in minimally invasive surgery which is laparoscopic and robotically. I guess that would be for the inpatient.
And outpatient, what I'm excited for is the fact that this drug with what appears to be lower side effects that we'd be able to give people pain free and out of the recovery room faster. So, any patient I do in an outpatient surgery center, I think, there would be a role for this drug because, again, we are limited in space by recovery room. And if we get back up in the recovery room, everything kind of slows down.
So, I do the majority of my patient cases in an outpatient surgery center, to be honest with you, and that's the trend nationally as more and more stuff is being done as outpatients and a big part of that is controlling costs. So, I would say almost all patients we do as outpatients would be good candidates for this drug.
Now, costs are interesting. In the hospital, it would get absorbed in what's called the DRG. And the hospital looks at costs somewhat, but not super strict because it seems to me, like in our hospital, that DRG payments are fairly large, and they don't micromanage us very much on if we're using drugs that are a little bit more expensive than others. Sometimes, a little bit, we will get pushback. That's mostly on antibiotics. And that's mostly so you're not changing the form of antibiotics in our area.
In the outpatient surgery center, the margins on the cases are much smaller, and so costs are looked at more. So, I don't have any idea of what this drug is going to come out as cost-wise. But that would be looked at a little more as far as do we see a benefit from that.
But, again, I think most of us at the surgery center look at the bigger picture. So, if a drug does cost a little more, but people are happier getting out of the surgery center faster and we're more efficient, then the overall efficiency, I think, would far outweigh the cost of the drug.
An example of that is when IV Tylenol came out. That's a lot more expensive than oral Tylenol, but yet we use it quite a bit because we see a benefit with that drug, even though the cost is more.
So, I hope that answers your question.
Jason Butler (24:19)
That's great. Thank you very much. And thanks for taking the questions.
Carrie Bourdow
Thank you. Thanks, Jason.
Operator
The next question is from Douglas Tsao of H.C. Wainwright. Please go ahead.
Douglas Tsao (24:29)
Hi, good morning. I guess my first question is for Dr. Beard. In terms of you think about your overall patient population, both inpatient and outpatient, or you could address them separately, what percentage of them do you think fall into this high risk category and would be candidates for use once it is eventually hopefully approved?
Carrie Bourdow
Great. Thanks. Thanks, Doug. Great question. Dr. Beard, did you hear the questions, the percent of high-risk patients. Yeah?
Timothy Beard
Yeah. So, that percent goes up daily, it seems. I don't know. That was a real patient example that I gave. She was 5′1″, 325 pounds. So, that was an extremely difficult case and extremely difficult post-operative recovery. So, I would think, in our hospital, when this drug gets approved in August, we'd probably be able to get it to the P&T pretty fast, would be my guess.
And you probably start using it on higher risk patients. So, people with pulmonary issues, people that are at risk for nausea and vomiting. For example, I do a lot of laparoscopic foregut surgeries, which are called Nissen fundoplication or paraesophageal hernia repairs, mostly for heartburn and reflux, and if those patients retch or vomit, it can totally disrupt the wrap that you've done.
So, I would say, if I had to give a number of inpatients that I would say are what I would consider higher risk and that this drug is just tailor-made for, it'd put it probably at 50% or 60%. Unfortunately, I don't have a practice where I can operate on all this in healthy patients all the time, I wish. But this doesn't exist in reality.
Again, in the outpatient, these are healthier patients by definition. We don't do anyone over an ASA 3 in an outpatient surgery center, so they're healthier. But I think their benefit, again, it's a little different. It's not so much for their post-operative risk. The drug would be used for its what appears to be lower side effect profile and patient satisfaction and ease of getting them to our system.
Douglas Tsao (26:45)
And then, just one follow-up. Or two follow-ups, one for Dr. Beard. I know you mentioned you're often treating – sort of taking a polypharmacy approach. Just curious what drugs oliceridine alone would be able to replace. And then, just a question for Carrie in terms of TRV045, the S1P, which are going into epilepsy. Just curious, how it was epilepsy was the first indication selected for development? Thank you.
Carrie Bourdow
Great. Yeah. Tim, I'll let you start on oliceridine.
Timothy Beard (27:19)
Sure. So, we've developed these massive what are called ERAS pathways after surgery for a lot of our surgeries, which is Enhanced Recovery After Surgery. I'm sure you're familiar with them. And in that pathway, we do everything we can to optimize patients postoperatively. So, let's say I do a colectomy on someone, take out a colon for colon cancer. We obviously do a lot of stuff pre-op for those patients, but postoperatively even though they may get tap blocks or these rectus sheath blocks, they all get IV opioids. So, the drugs we give to counteract IV opioids, we give a drug called alvimopan or Entereg, which is a peripheral acting new opioid receptor antagonist, which blocks the side effects that opioids have on the gut. So, opioids cause an ileus where they cause the gut not to move. You can't pass gas or stool. So, you get that drug. We give a whole bevy of antiemetics, probably at least three different antiemetic to prevent the nausea and vomiting, including sometimes we give Decadron in surgery or Zofran or Phenergan or Compazine, any of those we can give to stop the post-operative nausea and vomiting.
We also then are super aggressive with our respiratory care on these patients. So, we get a respiratory therapy consult, do incentive spirometers and may or may not give them nebulizers if they need it. So, I think those are the three sort of main areas that we were giving drugs to counteract the side effects of opioids.
Carrie Bourdow
And it sounds like – it's difficult for you right now to say what oliceridine may replace. You've got to get it in your hands, I think, and use it, right, is really Doug's question around what potentially oliceridine could replace.
Timothy Beard
Right. We're hoping – because, yeah – and what I tried to mention in my talk is that when you give so many different drugs to the polypharmacy that the compliance to that regimen is fairly low. That's what we're finding out with our ERAS protocol, is that we give all these different drugs and then people actually don't really get them scheduled because it's too much, the compliance is fairly low. So, yeah, we don't know. That's why I'm excited for this drug to get approved to try it to see how much we can eliminate because anything we can do to simplify it would be great.
Carrie Bourdow (29:42)
Thank you. Thank you. And then, Doug, to follow-up on your question on S1P, so quick reminder, and I'll turn it over to Mark to talk specifically about epilepsy, but there are other areas that we've studied with TRV045 or in the process of looking at. Chemo-induced peripheral neuropathy is another area that we've looked at on the animal data. And then, epilepsy was really – Mark is going out and talking to folks that are involved in looking at epilepsy drugs and epilepsy trials. So, Mark, I'll let you talk a little bit about…
Mark Demitrack (30:18)
Doug, it's a great question. And as you know, we've talked in the past, the S1P target is really quite interesting because of its broad representation in the CNS. So, really, the challenge for us is more focused since there's an enormous number of targets that are of potential interest.
And as Carrie mentioned, most of our early work was focused on chemotherapy-induced peripheral neuropathy in rodent models. That's one of the best studied animal models for the S1P system. But because of S1P localization on cell types in the brain, particularly glial cell types or astrocytes, it has demonstrable impact on various measures of membrane stability. And as a result, people became interested in the idea of exploring it in epilepsy models. And although it's not as well studied as the CIPN work, there has been some animal work done with some of the available S1P ligands, like fingolimod, for example. Now, you know that fingolimod is a non-selective S1P modulator and it also is accompanied by peripheral immunosuppression.
The S1P1 receptor target, which is what 045 is directed at, is a bit more selective to the CNS receptors and it also is absent in immunosuppression in our studies to date. So, it allows us to build on some of the literature that exists for the epilepsy target in animal models with earlier tool compounds. And that really is kind of the thing that prompted our interest.
The collaboration with EPSP emerged from those discussions. EPSP program is a longstanding, well regarded preclinical screening program that's sponsored by NINDS through the NIH. It's been in existence for about 30 years and has actually shepherded along several pretty key anti-epileptics to the market in their experience. So, we're pretty gratified that in our discussions that we've engaged in this program. So, further updates in the future.
Carrie Bourdow
Thank you. Thanks. Great.
Operator
This concludes the question-and-answer session. I would now like to turn it back to Carrie Bourdow for closing comments.
Carrie Bourdow
Great, thank you. And thank you for your questions. Thank you to Dr. Beard for addressing the questions. We appreciate that.
Let me close with some of the key points that you heard today. First, we've executed on our plan. We did what we said we were going to do. We resubmitted the NDA for oliceridine, got confirmation from FDA that the submission was complete, and we also advanced the pipeline, as we carefully managed our expenses.
I'd like to add my thanks to the team for their hard work and commitment. We expect 2020 to be a transformational year for Trevena. With the oliceridine NDA now under FDA review, we're preparing for expected approval in August. And we're also going to continue to make progress on the pipeline. So, I will continue to provide updates as the year progresses. Thank you again for joining us this morning on the call.
Operator
This concludes today's teleconference. You may disconnect your lines at this time. Thank you for your participation.

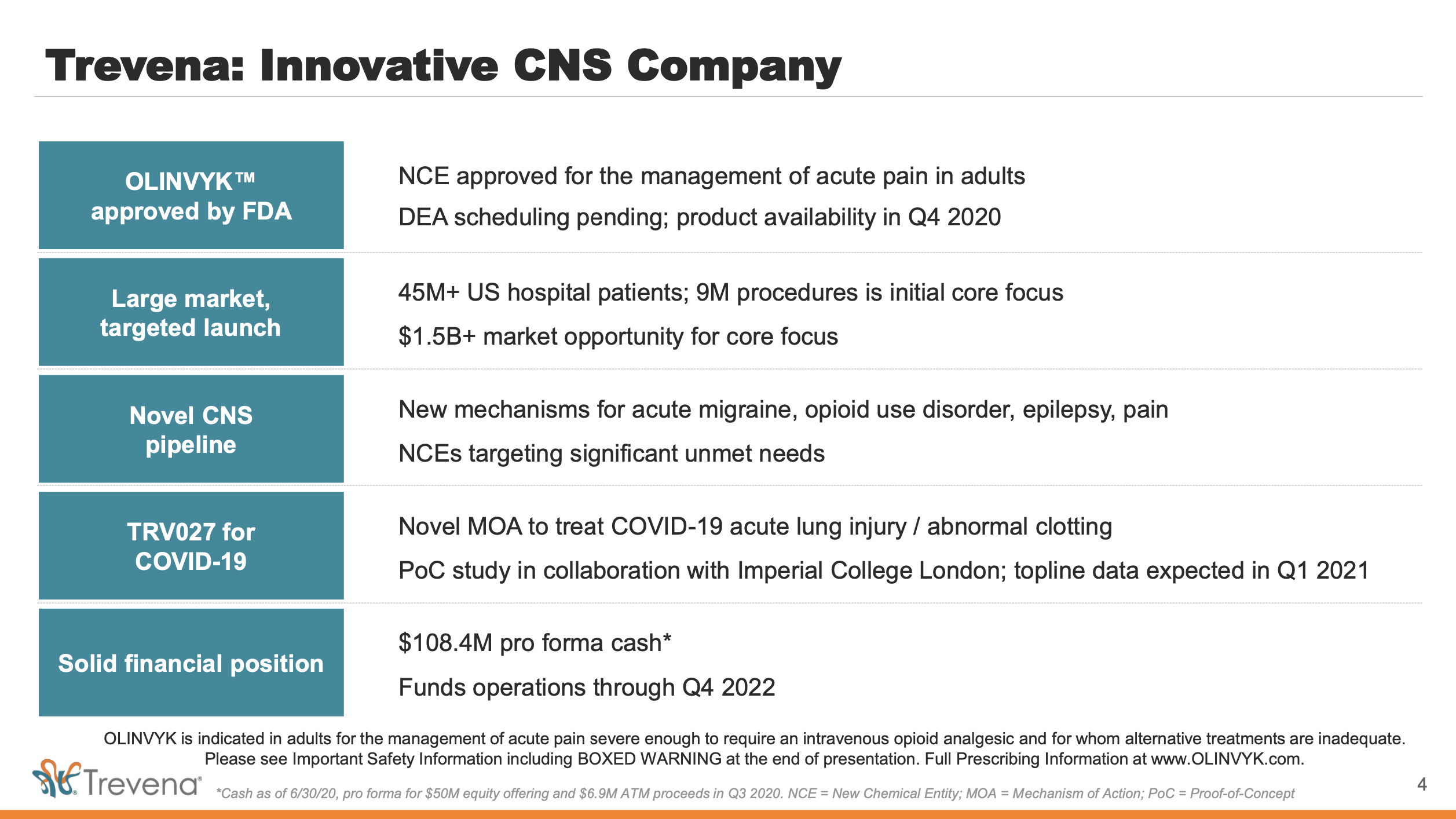{kind=link}
{kind=link}